Sameen Meshkin and Moosa Zaidi
Mass Eye & Ear
Diabetic Macular Edema Session
The Macula 2025 session on diabetic macular edema (DME) was moderated by Drs. Mira Sachdeva, Allen C Ho, and Ishrat Ahmed
Current Role of Fluorescein Angiography in DME
First, Dr. Yannis Mantas Paulus presented on the current role of fluorescein angiography (FA) in DME. He highlighted the association of peripheral pathology that can be captured on ultra-widefield imaging with a higher risk of diabetic retinopathy (DR) progression. He also discussed the utility of focal laser, guided by FA, in reducing the anti-VEGF injection burden for patients. His recent work finds 77.48 mm2 area of nonperfusion on Optos UWF FA to be a useful threshold in predicting progression to PDR. More generally, he postulated that it may soon be possible to quantify the risk of progression to PDR associated with a particular FA. Finally, he discussed the use of smartphone-based retinal imaging and AI for expanding access to DR screening for primary care offices and low-resource settings.
New Agents for DME: Just Durable or More Durable
Next, Dr. Judy E Kim reviewed data on the durability of two newer agents for DME: aflibercept 8 mg and faricimab 6mg. The PHOTON trial compared aflibercept 8 mg injected every 16 weeks, aflibercept 8 mg injected every 12 weeks, and aflibercept 2 mg injected every 8 weeks. All three arms achieved similar gains in BCVA at 96 weeks. Furthermore, 88% of patients in the 12 week interval arm and 84% of patients in the 8 week arm were able to be maintained on their initial injection interval, without a need for interval shortening per pre-established criteria. Thus, aflibercept 8 mg does appear to be more durable than aflibercept 2 mg. The YOSEMITE and RHINE trials compared faricimab 6mg injected every 8 weeks (RHINE) or under a Treat and Extend protocol (YOSEMITE) to afliberecept 2 mg injected every 8 weeks. Data from these trials similarly support the greater durability of faricimab compared to afliberecept 2 mg. They also suggest that faricimab, a bispecific antibody against both Ang-2 and VEGF-A, may be more effective in reducing inflammation and ERM formation. Thus, overall, both alfiberecept 8 mg and faricimab 6 mg appear more durable than afliberecept 2 mg, but cannot be compared without a head-to-head trial.

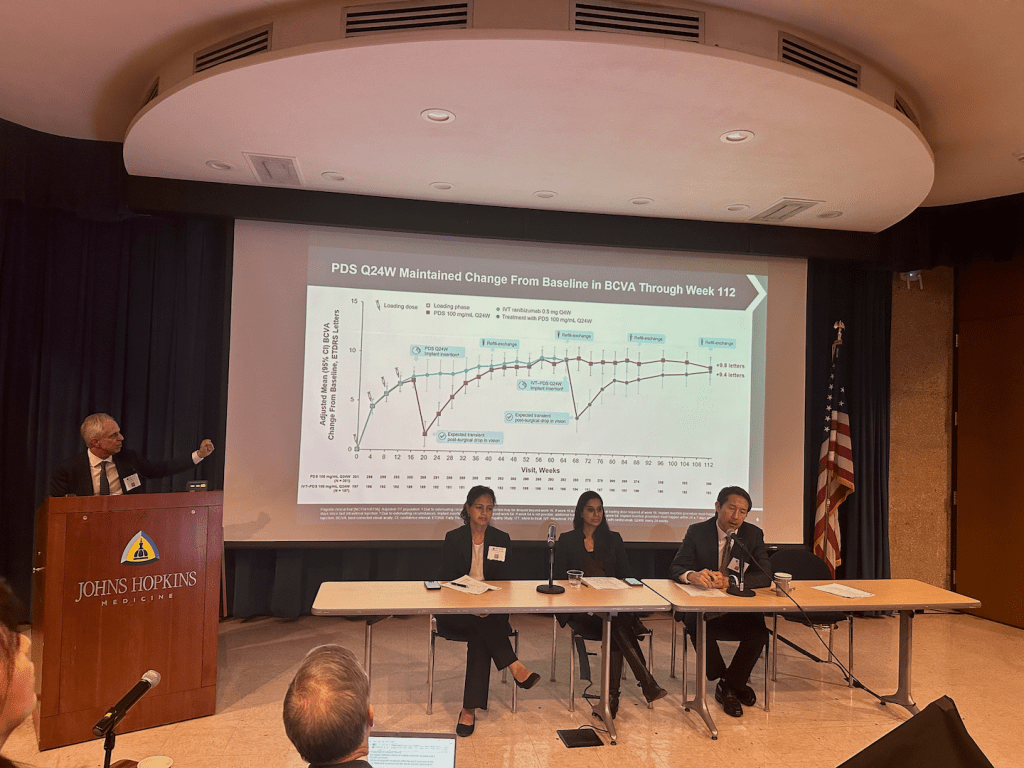
Port Delivery System Updates for DME
Highlighting a different avenue for reducing injection burden for patients with DME, Dr. Carl D Regillo presented 2-year data from the phase 3 Pagoda trial for a ranibizumab Port Delivery System (PDS). Implantation of the PDS with refill every 24 weeks was compared to monthly intravitreal ranibizumab 0.5 mg injections. With a high rate of study completion, the study demonstrated noninferiority of the PDS arm in maintaining vision gains over 2 years, with similar BCVA and CST improvements between the two arms. Three key potential adverse events which were of particular interest, implant dislocation, endophthalmitis, and retinal detachment, occurred in 0.2%, 0.7%, and 0.7% of participants respectively. No new safety signals were identified in the study. Thus, the ranibizumab PDS presents a promising new treatment option for DME.

AI in DME: At Its Infancy or A Flash in the Pan
Dr. T. Y. Alvin Liu discussed the potential role of AI in the evaluation and treatment of DME. He presented six possible applications: detection and classification of DME in color fundus photos (CFPs), prediction of visual acuity from CFPs, detection of DME in OCT images, prediction of visual acuity from OCT, quantification of DME and associated biomarkers in OCT, and prediction of treatment response to anti-VEGF injection. In addition to highlighting recent publications in each application area, Dr. Liu discussed potential real-world use cases. For example, he proposed detection of center involving DME (CI-DME) and prediction of visual acuity from CFPs could be used for at-home or remote monitoring that would expand access and reduce the required frequency of in person visits. With this focus on real world applications, Dr. Liu cautioned that although many applications of AI to DME have been published, only a selected few are likely to have a real-world impact, and scaling of these select few applications will require innovations in clinical workflows and payment models.

Approaches to Prevent Worsening of Diabetic Retinopathy
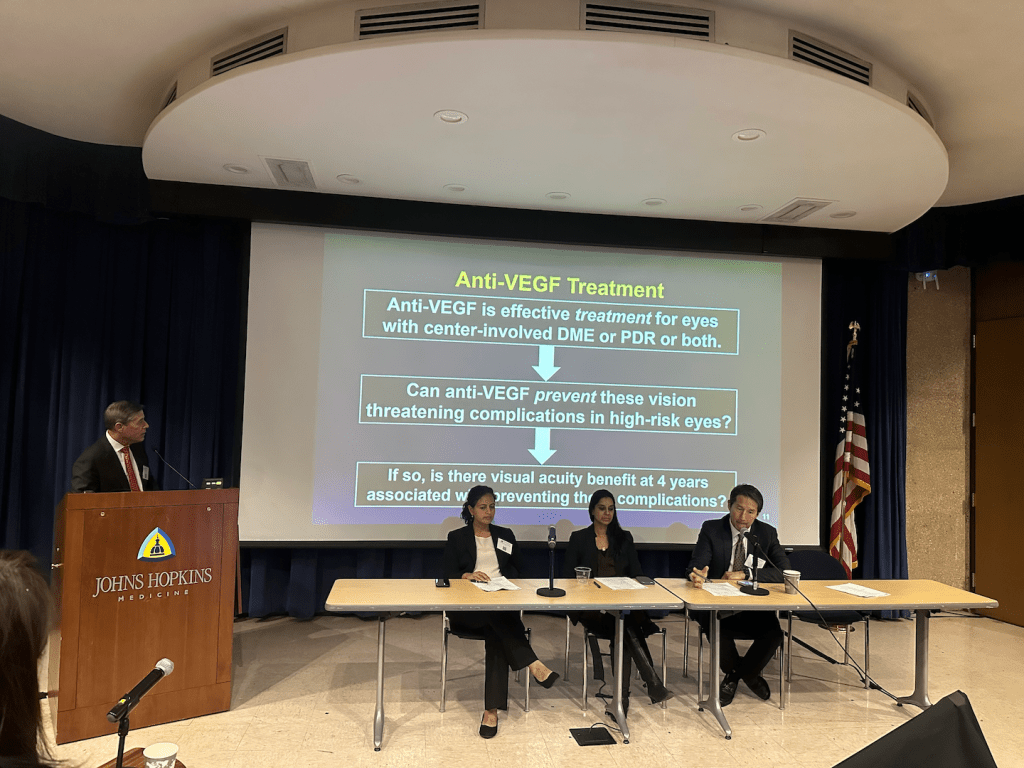
Finally, Dr. Neil Bressler discussed three approaches to preventing worsening of DR. First, Dr. Bressler highlighted the landmark 1993 NEJM paper by the Diabetes Control and Complications Trial (DCCT) Research Group and a 2008 follow up study which show compelling evidence that intensive anti-diabetes therapy aimed at near normal glycemia prevents worsening of DR Thus, encouraging patients to work with their general medical providers to optimize glycemic control is a crucial means of preventing DR worsening. Next, Dr. Bressler highlighted two placebo-controlled clinical trials (FIELD and ACCORD) that demonstrated a beneficial effect of fenofibrate on DR. Noting multiple reasons for currently limited adoption of fenofibrate for treatment of DR despite this data, Dr. Bressler presented an active DRCR Retina Network multicenter randomized control trial that aims to further investigate the effectiveness of fenofibrate in preventing DR worsening and to potentially disseminate prescribing guidelines. Finally, Dr. Bressler reviewed data from Protocol W which demonstrate that while prophylactic, early initiation of aflibercept injection in patients with moderate to severe NPDR does reduce the incidence of CI-DME and PDR, it does not at 4 years achieve superior visual outcomes compared to standard observation and treatment.

The five excellent talks were followed by a Question and Answer session, which began with a discussion of what anti-VEGF agent practitioners prefer as first line for DME. Dr. John Thompson noted Avastin becoming harder to access. Dr. Judy Kim and Dr. Neil Bressler expressed support for aflibercept as first line, with Dr. Kim noting that a high percentage of patients started on Avastin will require conversion to aflibercept and that first-line aflibercept is increasingly being covered by payors. Responding to a question about the tradeoffs associated with a PDS, Dr. Carl D Regillo suggested that a PDS could selectively be the preferred choice of patients with aggressive disease requiring more frequent injections. During a discussion of the potential effects of Ozempic on DR, Dr. Bressler highlighted the ongoing Focus trial. Finally, Drs. Allen C Ho, T. Y. Alvin Liu, Lee M Jampo, and others, all contributed to a discussion of the need to pair technological advancements with improvements and innovations in healthcare models and healthcare access in order to fully realize prevention of DR associated vision loss.
Proliferative Diabetic Retinopathy Session
Drs. John Thompson, Bailey Freund, and Richard Rosen moderated the Proliferative Diabetic Retinopathy session during which two talks were given by Dr. Lee Jampol and Dr. Dean Eliott.
Dr. Jampol’s talk, Proliferative Diabetic Retinopathy (PDR): Anti-VEGF, PRP, or Both began with a summary of ~75 years of research that guided us to the current point in our understanding of PDR treatment with laser and intravitreal anti-VEGF injections.
His talk focused on four studies: PROTEUS study (from the EVICR Study Group), CLARITY study, a record database analysis (TriNetX) as well as DRCR network Protocol S (2- and 5-year results).
Several factors were considered when attempting to reach a conclusion as to which modality, PRP or anti-VEGF, is superior: efficacy, safety, cost, cost effectiveness, number of visits and testing sessions required, number of injections and lasers administered, doctor time, patient time, and compliance. He also briefly mentioned several additional outcomes that merit further study: visual field changes, development of DME, need for vitrectomy due to vitreous hemorrhage, and tractional retinal detachments (TRD).
The PROTEUS study compared ranibizumab + PRP vs. PRP alone for high-risk PDR. The study showed ranibizumab + PRP was more effective than PRP alone for neovascular regression over 12 months.
Next, he discussed the CLARITY study which compared clinical efficacy of aflibercept vs. PRP for BCVA in patients with PDR. The study showed aflibercept had superior visual outcomes when compared to PRP at 1 year, further supporting its role as an effective treatment option for PDR.
He then turned our attention to a retrospective study using the TriNetX database (an aggregated electronic health records network), which evaluated whether the order of PRP and anti-VEGF injections affects outcomes in patients with PDR. The study showed treatment with PRP first and subsequent anti-VEGF injection was associated with higher rates of pars plana vitrectomy (PPV) (for vitreous hemorrhage and TRD) at 5 years compared with patients treated with anti- VEGF injection and subsequent PRP.
Finally, Dr. Jampol reviewed data from the DRCR.net Protocol S trial which demonstrated that ranibizumab therapy for PDR is non-inferior to PRP at 2 years for change in visual acuity from baseline (5-letter non-inferiority margin). In terms of visual field data, PRP had larger initial visual field losses than ranibizumab, however, beginning around 2 years and progressing to 5 years, the ranibizumab group had progressively worsening visual field losses nearly catching up to the losses noted with PRP.
To conclude, Dr. Jampol reminded the audience of a future DRCR trial (Protocol P) which will evaluate vitrectomy and endolaser vs. anti-VEGF and laser in PDR.

Dr. Dean Eliott’s talk, Evolving Indications for Surgery in PDR, traced the evolution of vitrectomy surgery from its initial introduction by Dr. Robert Machemer in 1971 to the present day. He highlighted the key principles of diabetic vitrectomy: 1) to clear media opacities 2) to elevate and excise posterior hyaloid and all associated fibrovascular proliferations 3) to maintain hemostasis, 3) to identify retinal breaks, 4) to perform thorough endolaser, 5) to perform possible retinectomy, and 6) to administer tamponade agent.
The Diabetic Retinopathy Vitrectomy Study (1985) showed that early vitrectomy for vitreous hemorrhage (defined as before 6 months) resulted in better visual and anatomic results than deferred vitrectomy (waiting over 1 year). Fast forwarding to 2024, the Moorfields Retrospective Study showed that early vitrectomy (before 6 weeks) resulted in better visual acuity and fewer complications than delayed vitrectomy (waiting > 6 weeks) in vitreous hemorrhage secondary to PDR.
He reviewed the standard of care in 2025 for new, dense vitreous hemorrhage in PDR (with minimal or no traction on ultrasound): to perform anti-VEGF injection with ~1 month follow-up, followed by PPV if no improvement. This is a general paradigm with additional considerations such as whether the patient has had PRP and the status of the fellow eye.
Dr. Eliott reviewed the evolution of indications for vitrectomy surgery in PDR which today encompasses: premacular/subhyaloid hemorrhage, dense vitreous hemorrhage, TRD involving the fovea, combined TRD-rhegmatogenous retinal detachment (RRD), severe fibrovascular proliferation, ghost cell glaucoma, DME with taut hyaloid or vitreomacular traction, fovea- threatening TRD, and rarely, DME without traction and vitreopapillary traction.
He described the utility of focal posterior retinectomy in cases of contracted fibrovascular plaque with adjacent break while reserving use of large peripheral retinectomy for the less common PDR presentations with extensive diffuse retinal contraction.
Finally, Dr. Eliott reviewed the many technological enhancements that have guided this evolution in surgical approach, namely, enhanced visualization, new vitrectomy machines, new adjuvants, illuminated curved laser probe, and better smaller-gauge cutters and scissors.


Read All Atlantic Coast Retina Club / Macula 2025 Articles:
Mystery Cases 1 & 2
Mystery Cases 3 & 4
Mystery Cases 5 & 6
Mystery Cases 7, 8, 9
Imaging, GA, and IRDs
Keynote Lectures
DR and DME
Choroidal Neovascularization
Retinal Vascular Diseases
Ocular Oncology
Special Topics & Women in Retina