Henry W. Zhou, MD, MS
Mass Eye and Ear, Boston, MA
The Surgical Case-Based Panel Discussion at ASRS 2025 featured leading vitreoretinal surgeons as they addressed challenging surgical scenarios. Dr. J. Michael Jumper from West Coast Retina Medical Group moderated the session, with panelist contributions from Dr. Lizzy Rossin (Mass Eye and Ear), Dr. Mrinali Gupta (Retina Associates of Orange County), Dr. Kevin Blinder (The Retina Institute), Dr. Alay Banker (Banker’s Retina Clinic and Laser Centre), and Dr. Wei Chi Wu (Chang Gung Memorial Hospital).

Case 1: Epiretinal Membranes
The panel began with a 56-year-old patient presenting with epiretinal membrane, outer retinal disruption, and 20/40 vision. Dr. Rossin advocated for surgery only in symptomatic cases. Dr. Gupta took a measured approach and would not recommend surgery during the initial consultation but would proceed if symptoms developed, regardless of visual acuity measurements. Dr. Wu favored watchful waiting until metamorphopsias became more prominent.
Case 2: Membrane Peeling Techniques
Discussion then shifted to surgical approaches for membrane peeling. Dr. Blinder shared his preference for brilliant blue dye combined with the pinch-and-peel technique. He also advocated for removal of the ILM after ERM peeling. Dr. Banker uses double staining and frequently achieves simultaneous ILM-ERM removal. Other panelists echoed support for the pinch-and-peel method.
Case 3: Managing Lamellar Macular Holes
A patient with a lamellar macular hole and 20/40 vision highlighted the importance of natural history and careful counseling. Dr. Blinder leaned toward extended observation for the case as presented, though he would perform macular hole surgery (via a standard approach) for symptomatic patients. Dr. Rossin stressed the significance of disease progression and is more inclined to operate when deterioration is evident. She emphasized thorough preoperative counseling about risks, particularly the potential for full-thickness hole development and gas tamponade requirements. Dr. Gupta highlighted the critical distinction between tractional and degenerative lamellar holes, noting poor surgical outcomes with the latter. Dr. Banker described his approach using foveal-sparing ILM techniques with gas tamponade.
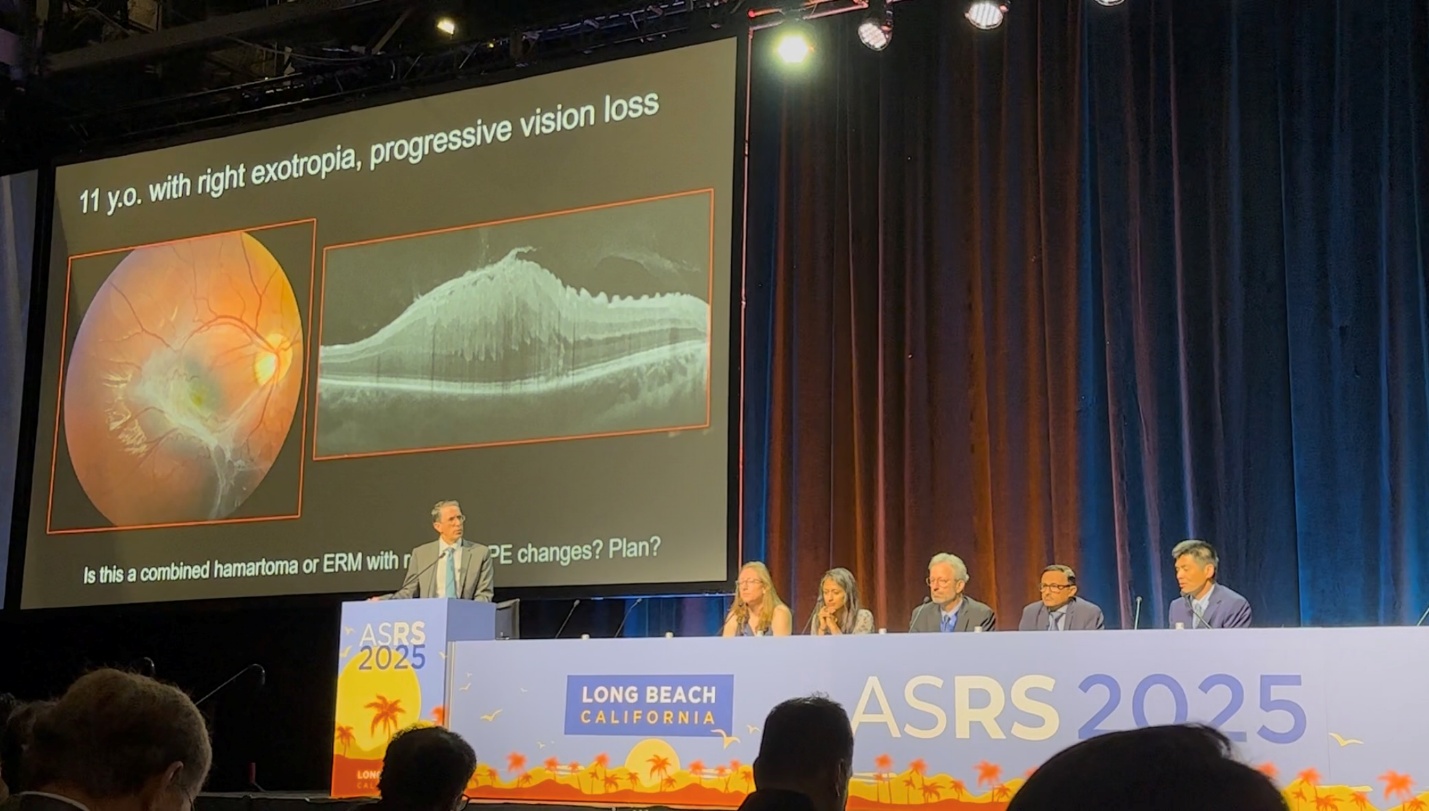

Case 4: Combined Hamartoma of the Retina and RPE
An 11-year-old girl with progressive vision loss and negative workup for toxocariasis and neurofibromatosis prompted Dr. Wu to suggest testing for FEVR, Coat’s disease, Stickler syndrome, and uveitic conditions. He pointed to the grayish fundus appearance and characteristic see-saw appearance of the retina on OCT as suggestive of combined hamartoma of the retina and RPE. Dr. Banker would consider surgery for progressive symptoms but cautioned about the adherent nature of these membranes. Dr. Jumper confirmed the surgical challenge, noting difficult membrane peeling and hyaloid separation in this case.
Case 5: Vitreomacular Traction
A 69-year-old man with VMT and distortion led Dr. Blinder to recommend observation—what Dr. Jumper memorably termed “MICCO: meticulous inactivity coupled with cat-like observation.” Dr. Gupta reserved surgery for patients significantly troubled by their symptoms, and her surgical approach would be identical to a standard macular hole surgery.
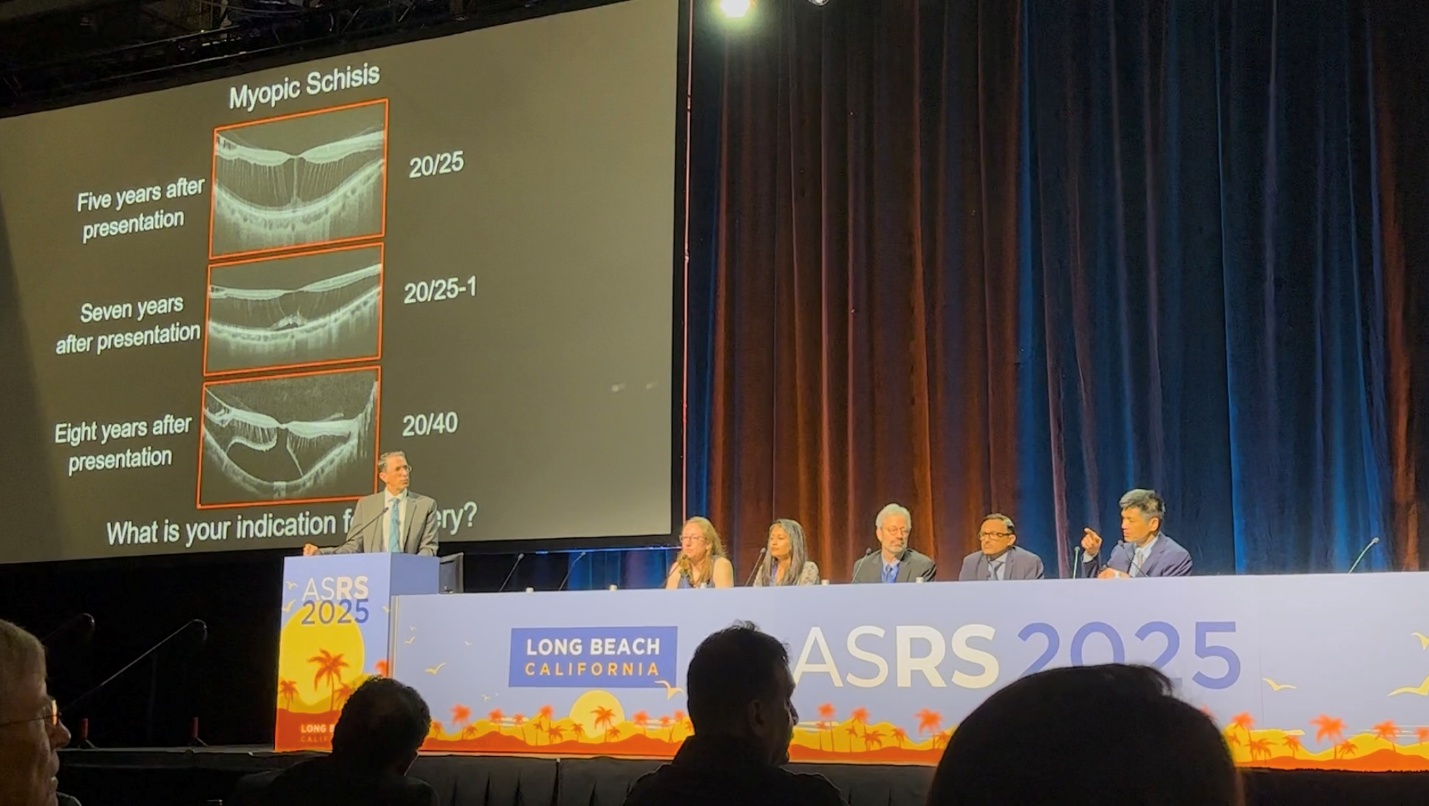

Case 6: Myopic Schisis
The panel was shown eight years of progression in a case of myopic schisis that eventually developed sub-foveal retinal detachment. Dr. Wu noted the potential for gradual visual decline, reserving surgery for foveal detachment with progressive vision loss. His technique involves fovea-sparing ILM peel.
Case 7: Concurrent Cataract and Macular Hole
A 68-year-old man presented with both a 2+ nuclear sclerotic cataract and full-thickness macular hole. Dr. Gupta and Dr. Rossin preferred addressing the macular hole first, deferring cataract surgery. Dr. Banker noted that while he doesn’t perform cataract surgery himself, combined procedures are standard practice among Indian surgeons. Dr. Wu mentioned he doesn’t require face-down positioning due to compliance concerns. Dr. Jumper stressed the importance of avoiding face-up positioning.
Case 8: Large Macular Hole Repair Options
For large macular holes, Dr. Wu discussed autologous retinal transplants and amniotic membrane use. Dr. Banker shared experience with sub-Tenon’s capsule repairs. While Dr. Blinder hadn’t found success with retinal transplants, he reported good outcomes employing sub-Tenon’s capsule transplants. Despite Dr. Jumper’s limited experience with autologous transplants, his results showed promising anatomic and functional outcomes.
Case 9: Myopic Macular Hole with Detachment
Dr. Gupta outlined her approach: PPV, PVD induction, ILM peel, and distal drainage retinotomy. Dr. Rossin, however, avoids drainage altogether as fluid-air exchange adequately covers the hole, with fluid typically resolving by postoperative day one. Dr. Wu supported this drainage-free approach.
Case 10: Optic Pit Management
A case of optic pit with subfoveal fluid led Dr. Banker to advocate for observation, as many resolve spontaneously. For persistent, symptomatic cases, he would perform a temporal ILM flap for coverage of the pit with fluid-gas exchange. Dr. Blinder humorously noted he wouldn’t use punctal plugs for optic pit closure, despite promising results presented the previous day.
Case 11: Vitreous Hemorrhage
Dr. Gupta typically observes uncomplicated vitreous hemorrhage closely, proceeding to surgery within two weeks for fundus-obscuring, non-clearing hemorrhages. Dr. Rossin treats vitreous hemorrhage without posterior visualization like macula-on retinal detachment, expediting surgical intervention.
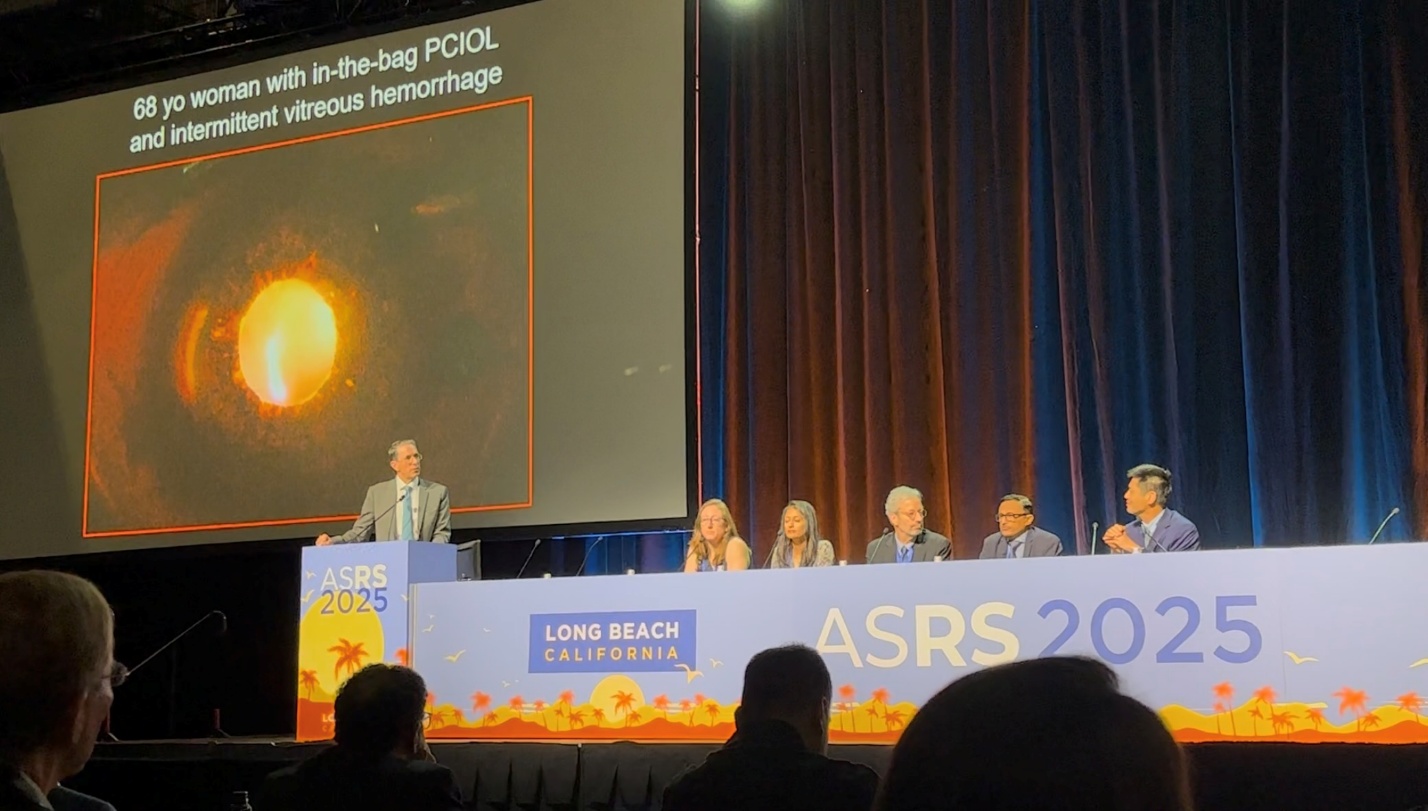

Case 12: Iris-Haptic Chafing
A 68-year-old woman with intermittent vitreous hemorrhage and haptic-shaped transillumination defects prompted discussion of IOL complications. Dr. Wu has observed haptic perforation through capsular bags causing iris chafing. Dr. Gupta noted increased iris-haptic chafing risk in eyes with compromised zonular support, even without capsular bag perforation.
Case 13: Anterior Migration of Steroid Implants
A case of eye trauma led to a fluocinolone (Yutiq) implant migrating into the anterior chamber. Dr. Rossin acknowledged that while Ozurdex would pose greater concerns, she’d schedule surgery within weeks. She avoids steroid implants in eyes with IOLs that might permit anterior migration. Dr. Blinder removed a similar Ozurdex case within one week. Dr. Jumper classified anterior chamber Ozurdex as an ophthalmic emergency.


Case 14: Retinal Detachment and Keratoprosthesis
Dr. Rossin detailed technical considerations for retinal detachments in KPro cases, placing ports 8mm from the optic center (despite some recommendations for 9mm), given the possibility of implant decentration. She appreciated the consistently clear view from the Type 1 Boston KPro. She noted that pre-existing glaucoma drainage devices often cause rapid gas disappearance, leading her to prefer silicone oil.
Case 15: Acute Retinal Necrosis
The final case involved ARN progressing to detachment with multiple breaks. Dr. Banker, drawing from extensive experience, recommended complete vitrectomy, triamcinolone-assisted vitreous visualization, 5000cSt silicone oil, and 360-degree laser barrage without scleral buckling. Dr. Wu wouldn’t perform prophylactic PPV but would initiate oral acyclovir and intravitreal foscarnet/ganciclovir. Dr. Rossin emphasized comprehensive 360-degree laser or barricading all lesions, as necrotic areas invariably develop breaks.
Conclusion
Through these fifteen cases, the expert panel shared nuanced approaches to complex vitreoretinal pathology. Their collective wisdom highlighted both surgical pearls and potential pitfalls, offering attendees valuable insights gained through years of clinical experience. The discussion underscored how surgical decision-making often requires balancing multiple factors—patient symptoms, disease progression, anatomic considerations, and technique selection—to achieve optimal outcomes.